
4.2: Module 10 – Gender Through a Clinical Psychology Lens
- Page ID
- 64425
Module 10: Gender Through a Clinical Psychology Lens
Module Overview
If you’ve taken Abnormal Psychology, you already know that there are discrepancies among diagnosis rate of mental health disorders between men and women. These differences have been attributed to biological differences, environmental differences, as well as methodological differences in data collection and symptom description. Therefore, the focus of this Module is to identify gender discrepancies amongst clinical psychology disorders and discuss possible explanations why these differences occur.
Module Outline
- 10.1. Methodological Artifact
- 10.2. Clinical Disorders
- 10.3. Suicide
- 10.4. Gender and Mental Health Treatment
Module Learning Outcomes
- To understand how methodological artifact contribute to the gender bias in diagnosis of mental health disorders
- To identify the gender discrepancies in rate of diagnosis for Major Depression Disorder, Anxiety Related Disorders, PTSD, and Eating Disorders
- To understand various cognitive, social, and biological variables that contribute to the gender differences in selected mental health disorders
- To understand the gender paradox of suicide
- To understand variables that contribute to gender differences in seeking mental health treatment
10.1. Methodological Artifact
Section Learning Objectives
- To increase understanding of how methodological artifacts contribute to gender bias in clinical psychology
- To increase understanding and identification of the types of clinician bias and how they impact diagnosis rate of mental health disorders
- To increase understanding of how response bias can impact diagnosis rate of mental health disorders
Before we discuss gender differences among clinical disorders, first we must discuss possible explanations of these differences aside from gender specific factors. There are three proposed theories regarding the difference in diagnosis rate between genders. The first two are suggestive of methodological artifact, or the belief that findings are not reflective of real-world data, but rather, an unintended consequence of methodological artefact (encyclopedia.com). Two methodological ways this can occur is through clinician bias and response bias. The final theory is that manifestation of symptoms are different among men and women, and instruments such as questionnaires are biased to these symptoms.
10.1.1. Clinician Bias
Have you ever met someone and made a judgement about them on the first meeting only to find out several days (months, years, etc.) later that your initial assessment of them was wrong? Unfortunately, this can also happen to clinicians. The diagnosis of a psychological disorder requires the clinician to gather information from the patient, interpret the information along with their own observations, and determine whether or not the patient meets criteria for a diagnosis. This assessment is usually completed within the first couple of sessions when clinicians have very little information about their patient. Clinicians are required to use their informal and subjective method of arranging client data to formulate a diagnosis and treatment plan (Grove et al., 2000). Unfortunately, through this process, clinician judgement and thus subjective bias may occur, thus influencing the diagnosis.
While there are many different types of clinician biases, among the most common are pathology bias, confirmatory bias, and over-confidence in clinical judgement (Moran & Tai, ??). Pathology bias suggests that clinicians may develop a bias to look for psychopathology as their clinical training and experience has emphasized finding disorders (Shemberg & Doherty, 1999). This is especially problematic in settings where individuals are influenced to display psychopathology such as in residential psychiatric settings.
Confirmatory bias also influences making inaccurate diagnoses as clinicians may have the tendency to only recall information that supports a diagnosis (Shemberg & Doherty, 1999). This is problematic in that clinicians will use this information to support their diagnosis, but not use data to refute their hypothesis, thus altering the true presentation of symptoms (Garb, 1998).
Finally, over-confidence bias occurs when clinicians become too confident in their subjective psychological assessments (Moran & Tai, ???). While rarely observed in new clinicians, this bias often occurs in seasoned clinicians who believe that more experience influences more effectiveness and accuracy in clinical judgment (Groth-Marnat, 2000).
10.1.2. Response Bias
To complicate the situation even more, in addition to clinician bias is patient response bias. A patient is responsible for providing information about themselves, including presenting symptoms. Unfortunately, some patients have a tendency to respond inaccurately or falsely to questions. While some of these errors may be unconscious, others may be intentional to prevent a specific diagnosis.
Studies have indicated that there are sex differences in attitudes toward various disorders such as depression. Individuals tend to associate depression as a “feminine” diagnosis, and thus, may lead male patients to underreport symptoms (Page & Bennesch, 1993). This also exceeds beyond depression as studies have shown both males and females are less willing to work with males than females with mental health disorders (Schnittker, 2000). Due to these cultural barriers, males may underreport their mental health symptoms to avoid stigmas.
10.2. Clinical Disorders
Section Learning Objectives
- To increase knowledge of prevalence rates of Major Depression Disorder in the US
- To increase understanding of the different variables that contribute to the gender differences in Major Depression Disorder
- To increase knowledge of prevalence rates of Anxiety Disorders in the US
- To increase understanding of the different variables that contribute to the gender differences in Anxiety Disorders
- To increase knowledge of prevalence rates of PTSD in the US
- To increase understanding of the different variables that contribute to the gender differences in PTSD
- To increase knowledge of prevalence rates of Eating Disorders in the US
- To increase understanding of the different variables that contribute to the gender differences in Eating Disorders
In this section we will explore a few clinical disorders with gender variations in both diagnosis rate, as well as symptom presentation. Discussing gender differences among all disorders is beyond the scope of this course, however, if you are interested to learn more about the prevalence rate of mental health disorders to can read the Abnormal Psychology OER textbook available within Pressbooks.
10.2.1. Major Depression Disorder
According to epidemiological research, there is no significant gender difference in Major Depressive Disorder (MDD) during childhood; however, by young adulthood, girls are twice as likely to be depressed as boys and report approximately twice as many depressive symptoms as boys, a difference that holds in both community and clinical samples, even when accounting for gender differences in help-seeking behavior (Nolen-Hoeksema, 1987). While this discrepancy holds true until age 55, research exploring gender differences of MDD prevalence rates in older adults is inconclusive, with some reporting a continuation of this discrepancy and others failing to report any difference between genders among older adults.
Researchers have identified several reasons why studying prevalence rates of disorders among males and females is difficult. One recurring reason is the difference in symptom presentation among genders. Kahn and colleagues (2002) evaluated male/female twins and depressive symptoms. Findings indicated that females reported more fatigue symptoms such as excessive sleep, slowed speech and body movements whereas males reported more hyperactive symptoms including insomnia and agitation. The findings are consistent with additional studies that indicate women more often report “passive” symptoms such as sadness, lethargy, and crying whereas men tend to associate depression with alcohol use. Due to the discrepancy in symptoms, it is not surprising that depression is more likely related to alcohol problems in males than females (Marcus et al., 2008). These findings are consistent when assessing for substance abuse disorders in general, with men more likely than women to not only have a substance abuse problem, but to also have a comorbid diagnosis of depression (Lai, Cleary, Sitharthan, & Hunt, 2005). This comorbidity not only complicated treatment for depression, but also willingness to seek mental health treatment in general.
10.2.1.1. Cognitive variables. Research regarding onset and treatment of depression routinely identifies the involvement of cognitive variables. Factors such as rumination and attributional style are among the most common factors assessed in gender research with regards to MDD. These factors not only explain differences in how males and females assess negative situations, but they also help clinicians to identify treatment interventions aimed specifically at factors contributing to an increase in depressive symptoms.
Rumination, or the response to negative moods by dwelling on them as opposed to problem-solving or distracting oneself, has been known to mediate the relationship between interpersonal stress and depression. More specifically, individuals with interpersonal stress and high levels of rumination report higher levels of depression than those with interpersonal stress and low levels of rumination (Lyubomirsky, Layous, & Nelson, 2015). When examining rumination with regards to gender, researchers routinely report that ruminating behaviors are more commonly observed in girls than boys (Johnson & Whisman, 2013; Rood et al., 2009; Grant et al., 2004). Given these findings, it should not come as a surprise that rumination also mediates depression within girls specifically, with girls experiencing higher levels of rumination also reporting higher levels of depression (Hamilton, Stange, Abramson, & Alloy, 2014). Interestingly enough, the relationship between males and rumination is the same, with males reporting higher levels of rumination also reporting significantly more symptoms of depression. Therefore, the pathway of increased ruminating thoughts leading to an increase of depressive symptoms appears to be the same in boys and girls, however, girls are more likely than boys to engage in ruminating thoughts in daily events.
Co-rumination, which is defined as a passive discussion of negative emotions and events with close friends is also observed more frequently in girls than boys (Barstead, Bouchard, & Shih, 2013; Bouchard & Shih, 2013; Rose, 2002). Unlike rumination where the relationship between increased ruminating thoughts and increased depressive symptoms did not differ between boys and girls, co-rumination appears to have a gender discrepancy. More specifically, engaging in co-rumination is correlated with increased depressive symptoms in girls, but NOT in boys (Rose, Carlson, & Waller, 2007).
In addition to ruminating on situations, one’s attributional style, or the way one interprets causes of events, has also been supported as a mediational variable to depression. More specifically individuals who attribute causes of events as internal, global, and stable are more likely to be depressed than those who view events as external, specific, and unstable (Morris, Ciesla & Garber, 2008). Researchers find that not only are girls more likely to attribute situations as internal, global, and stable, but they are also more likely to develop depressive symptoms from this attributional style than their male peers (Mezulis, Funasaki, Charbonneau, & Hyde, 2010). Thus, attributional style can predict depressive symptoms in girls but generally not in boys.
Another cognitive vulnerability that is liked to depression with regards to gender discrepancy is interpersonal orientation, or the tendency to behave in certain ways around people. Girls, more than boys, affiliate needs and define themselves more in relational terms (Brody & Hall, 2010; Rose & Rudolph, 2006). Because of this need to establish specific relationships, girls report both more frequent and more intense stress related to interpersonal orientation. Interpersonal orientation has also been linked to adolescent girls increased risk for developing depression due in large part to peer relationships. In fact, adolescent girls with friends who are depressed are more likely to develop depression; this finding has not been proven in their male peers (Giletta et al., 2011; Prinstein et al., 2005).
Why does interpersonal orientation not effect boys? The short answer: it does; however, girls, more than boys, are more concerned about what peers think of them, and therefore, effects girls more often than boys. In fact, deficits in peer approval are strongly associated with emotional distress in girls but not boys (Rudolph, Caldwell & Conley, 2005). Furthermore, girls are more reactive to relationship problems than boys. The combination of placing more emphasis on relationships, as well as being more responsive to relationship problems, may explain why there is a gender difference in depression even among young children and adolescents (Rudolph, 2009).
10.2.1.2. Stress and coping. In addition to cognitive vulnerabilities, stress and coping of various life events also contributes to the development of MDD. Observed gender differences in both frequency of and sensitivity to various life events is one possible explanation for the gender difference in depression diagnoses. Findings suggest that adolescent girls experience more stressful life events than boys AND rate these stressors with higher intensity than boys (Hankin, Mermelstein, & Roesch, 2007; Hammen, 2009; Seiffge-Krene, Aunola, & Nurmi, 2009). These findings are consistent in both the home and social setting. More specifically, girls who experience family discord report more symptoms of depression than boys and are at an increased risk for a depression diagnosis (Crawford, Cohen, Midlarsky, & Brook, 2001; Essex, Klein, Cho, & Kraemer, 2003). As stated above, girls also experience more stressful situations with peer relationships which has also been linked to increased depressive symptoms.
One explanation of the differences in depression rate and stress is the HPA axis. As previously discussed in Module 8, women are more likely to have a dysregulated HPA axis, and therefore, are more susceptible to negatively interpreting stressful situations than men (Nolen-Hoeksema, 2001). Additionally, hormonal changes are also known to trigger HPA dysregulation, thus making women more vulnerable to depression, particularly after stressful situations. The role of the HPA axis in combination with one’s coping style may predispose women to a susceptibility of depression.
10.2.1.3. Biological variables. We already discussed the role of sex hormones in the development of various behaviors in Module 8, however, it is worth noting that those hormones are also important in the gender difference of depression diagnosis. The biological changes during puberty are related to an increase in sex hormones; however, levels of sex hormones alone do not account for the difference in depression diagnoses (Angold, Costello, Erkanli & Worthman, 1999; Brooks-Gunn & Warren, 1989). Research indicates that the onset of puberty in girls is closely linked with depressive symptoms, with early onset puberty in girls being more at risk for developing depression; these findings have been mixed for boys, with no clear distinction of how onset of puberty may or may not affect depression symptoms (Crick & Zahn-Waxler, 2003; DeRose, Wright & Brooks-Gunn, 2006; Graber, Seely, Brooks-Gunn, & Lewinsohn, 2004; Mendle, Harden, Brooks-Gunn, & Graber, 2010).
One possible explanation for the relationship between early onset puberty and increased risk for depression is the fact that physical changes that occur during puberty are negatively perceived by girls (Stice, Presnell, & Bearman, 2001). Furthermore, secondary sex characteristics that occur during puberty are seen as less desirable, particularly in Western cultures that value thinness (Richards, Boxer, Petersen, & Albrecht, 1990). These values can lead to negative body image, which has also been predictive of increased depression symptoms (Ohring, Graber, & Brooks-Gunn, 20002; Stice & Bearman, 2001).
10.2.2. Anxiety Disorders
Anxiety disorders are the most common class of mental disorders with an estimated 19% of US adults experiencing some anxiety disorder in the past year (NIMH). Similar to depression, women are nearly twice as likely to develop an anxiety disorder than men across the lifespan across all anxiety related disorders. In fact, by the age of 6, anxiety levels in girls are twice as high as in boys (Howell, Brawman-Mintzer, Monnier & Yonkers, 2001). The current prevalence rate for any anxiety disorder for adult females is 23.4%, and 14.3% for males. This discrepancy is similar in adolescents, with overall higher rates of anxiety reported in adolescent samples (38.0% females, 26.1% for males).
When examining specific anxiety related disorders, women are more commonly diagnosed with panic disorder, agoraphobia, specific phobias, generalized anxiety disorder, and both acute and post-traumatic stress disorder (Gum, King-Kallimanis & Kohn, 2009; Bekker & van Mens-Verhulst, 2007; McLean, Asnaani, Litz, & Hofmann, 2011). However, the sex differences are less pronounced (and sometimes not statistically significant) for social anxiety disorder and obsessive-compulsive disorder (Bekker & van Mens-Verhulst, 2007; McLean & Anderson, 2009). Psychosocial, as well as genetic and neurobiological factors, likely contribute to the higher prevalence rate in women (Bandelow & Domschke, 2015).
The statistical difference between prevalence rates among genders is similar across all anxiety related disorders. Anxiety disorders represent a significant source of disability, especially for women. They are associated with more missed work days for women, but not men. This may be related to a greater comorbidity of anxiety disorders among women, and thus more severe psychopathology in general. Interestingly enough, men but not women, were more likely to visit a professional for either an emotional or substance use issue in the past year if they had an anxiety disorder (McLean, Asnaanin, Litz & Hofmann, 2011).
10.2.2.1. Biological variables. There are a few theories that attempt to explain the difference in prevalence rates among anxiety disorders. Anatomically speaking, there may be structural and functional sex differences in brain regions relevant to anxiety. More specifically, there may be a difference in male and female brains involvement in learning, memory, fear conditioning, and fear extinction. For example, a study exploring blood pressure and pulse found women are more physiologically responsive than men when presented with potentially anxiety provoking situations (Altemus, 2006). Researchers argue that this finding may indicate that women are more easily conditioned to fearful stimuli than males (Farrell, Sengelaub & Wellman, 2013). Given the appeared differences in fear conditioning, researchers have also argued that there may be a gender difference in fear extinction, thus impacting how the two genders respond to treatment of anxiety disorders.
Biologically, gonad hormones also play a role in the development and maintenance of anxiety symptoms. In women, estrogen and progesterone have been found to effect function of the anxiety related neurotransmitter systems, which in return, effect fear extinction (Lebron-Milad & Milad, 2012; Pigott, 1999). In fact, a study exploring the effects of long-term oral contraceptive use has been shown to alter the reactivity of the HPA axis in response to psychological stress (Biondi & Picardi, 1999). Testosterone also appears to play a role in the development of anxiety related symptoms. More specifically, testosterone has been linked to reduced responsiveness to stress and suppressing activity of the hypothalamic pituitary adrenal axis- the area responsible for our central stress response system. Although not as extensively researched as estrogen and progesterone, it does appear that gonad hormones likely account for some of the prevalence rate difference in anxiety related disorders.
10.2.2.2. Gender roles. One must also explore the role of gender roles in the development of anxiety related symptoms. When masculinity and femininity were measured on a single scale, higher levels of masculinity traits were negatively correlated with anxiety symptoms (Gall, 1969). Another study exploring the role of femininity and masculinity and anxiety symptoms found no relationship with femininity and anxiety symptoms; however, masculinity was negatively associated with anxiety and avoidance behaviors (Moscovitch, Hofmann & Litz, 2005). These findings were further supported when controlling for masculinity characteristics. More specifically, gender was not associated with avoidance in anxiety patients when controlling for masculinity characteristics, suggesting masculinity characteristics being largely responsible for these gender differences in avoidance and anxiety symptoms. All together, these studies implicate a relationship between masculinity traits and anxiety symptoms, with high levels of masculine traits regardless of gender correlating to lower reported anxiety symptoms. (Chambless & Mason, 1986).
Some researchers argue that due to gender stereotypes of anxiety symptoms, men may underreport symptoms, thus leading to a reporting bias. This is supported by an increase in fear reports in males (and not females) when examined via a physiological fear response. More specifically, although men were not reporting significant levels of anxiety related symptoms, physiological responses to stressful situations indicated heightened arousal that researchers linked to anxious behaviors (Pierce & Kirkpatrick, 1992). Researchers argue that due to social desirability, boys are more often encouraged to confront feared objects which leads to a greater exposure and extinction of fear responses, whereas girls are more supported in avoidance behaviors. This coupled with increased rumination may lead to more anxiety behaviors in girls across the lifespan (McLean & Anderson, 2009). Furthermore, women are at an increased risk of being exposed to traumatic events such as domestic abuse and sexual traumas, thus increasing the likelihood of developing anxiety related symptoms.
10.2.3. Posttraumatic Stress Disorder (PTSD)
Post-Traumatic Stress Disorder (PTSD) affects nearly 52 million Americans with a lifetime prevalence rate of 6.8%. Similar to both depression and anxiety disorders, women are more than twice as likely as men to develop PTSD at some point in their life. The lifetime prevalence rate for women is 9.7% and for men is 3.6% (NIMH,2019). While research on PTSD in children and adolescents is not as extensive as it is in adults, the minimal findings suggest a similar gender discrepancy with 8% of adolescent females meeting criteria for PTSD versus 2.3% of males.
Not only are women more likely to develop PTSD, but they also report a longer duration of posttraumatic stress symptoms (4 years for females vs. 1 year for males; Breslau, Davis, Andreski, Peterson & Schultz, 1997). This discrepancy may be due to the different types of traumatic events experienced. For example, men are more likely to experience traumatic events such as accidents, natural disasters, man-made disasters, and military combat whereas women tend to experience events related to sexual assault, sexual abuse, and domestic violence (Breslau & Anthony, 2007). Research indicates that despite differences in exposure to different stressors, women are still more likely to develop PTSD symptoms. For example, when men and women were assessed after a recent earthquake, women reported higher levels of posttraumatic stress symptoms than men (Carmassi and Dell’Osso, 2016). This study was also replicated with motor vehicle accidents (Fullerton et al., 2001) and terrorism (Server et al., 2008). So, if exposure to different stressful events does not account for the gender variance, then what does?
10.2.3.1. Biological variables. The natural biological response to a stress or threat involves a complex interaction within the HPA axis, allowing for the individual to prepare to the stressor, and then return to baseline once the threat is over. As we discussed in Module 8, cortisol, the main hormone produced in a stress response, is produced by the adrenal glands in activation of the HPA axis. While research on cortisol levels during stressful or threatening situations is mixed, the general pathway suggests that production of cortisol is increased when the individual is under distress in efforts to help the individual “fight or flight” the stressful event. During periods of prolonged stress, the HPA axis undergoes significant dysregulation in efforts to produce the cortisol response (Chrousos, 2009).
Assessment of basal cortisol levels in healthy men and women suggest that women have lower cortisol levels than men, however, women demonstrate a slower cortisol negative feedback than men suggesting women experience prolonged physiological stress than men (Bangasser, 2013; Van Cauter et al., 1996). When examining corticotropin-releasing factor (CRF), the hormone responsible for initiating the HPA axis response that ultimately releases cortisol, women show greater expression of CRF than men. This finding has also been replicated in animal studies that show a sex differences in CRF receptor binding, signaling, and trafficking. Therefore, the fact that women are twice as likely than men to develop PTSD may be due to an underlying biological predisposition (Bangasser, 2013).
Salivary cortisol levels also appear to be different in men and women with diagnosed PTSD. More specifically, women with PTSD appear to have lower levels of salivary cortisol that decreased over time, whereas men with PTSD have higher levels that increased over time (Freidenberg et al., 2010). Gender difference in cortisol levels in response to trauma is also observed in children with PTSD, with girl cortisol levels recorded higher than boys. Conversely, cortisol levels were higher in male but not female survivors of the World Trade Center attack (Dekel et al., 2013).
So, what accounts for the differences in basal cortisol and glucocorticoid negative feedback? Research indicates production of estrogen may account for these gender differences, which may also explain why girls initially have higher rates of cortisol but then as adults, have lower levels. Researchers have found via animal models that stress during adolescence (where there is a surge of gonadal hormones) impacts HPA axis reactivity and is associated with different behavioral responses in males and females (Viveros et al., 2012). Additionally, estrogen and menstrual cycle position have also been linked with intrusive memories (Cheung et al., 2013) fear inhibition and extinction (Glover et al., 2012, 2013) suggesting female hormone production may have a greater impact on women’s development of post-traumatic stress symptoms, as well as the biological mechanisms that facilitate stress response.
10.2.3.2. Cognitive variables. One of the diagnostic criteria symptoms of PTSD is intrusive recollection, or re-experiencing, of the traumatic event. Researchers have repeatedly found that these re-experiences, particularly the physiological reactivity related to the re-experiencing, were central to the development and maintenance of additional PTSD symptoms (Armour et al., 2017; McNally et al., 2017). Further studies found that increased re-experiencing of the traumatic event via dreams or distressing recollections initially following the trauma was predictive of PTSD six months after the traumatic event (Haag et al., 2017). Gender studies examining re-experiencing of symptoms identified women as having a higher level of both re-experiencing symptoms post-traumatic event, as well as a higher physical reactivity when remembering the incident (Fullerton et al., 2001; Stuber et al., 2006). Therefore, the fact that women report both increased re-experiencing and hyperarousal immediately following a traumatic event may explain why PTSD symptoms are more pronounced in women.
10.2.4. Eating Disorders
According to the DSM-V, there are three types of eating disorders- Anorexia Nervosa, Bulimia Nervosa, and Binge Eating Disorder. Anorexia nervosa involves the restriction of energy (i.e. food) that leads to a significantly low body weight for age, sex, and developmental status. These individuals have an intense fear of gaining weight or becoming fat, along with significant disturbance in their body evaluation. Bulimia nervosa involves recurrent episodes of binge eating followed by recurrent inappropriate compensatory behaviors in order to prevent weight gain. Finally, Binge Eating Disorder involves recurrent episodes of binge eating but do not engage in compensatory behaviors.
According to the National Eating Disorder Association, nearly 10 million American women and 1 million American men suffer from an eating disorder. Across all three disorders, women are more likely than men to be diagnosed with an eating disorder, however, the smallest gender discrepancy is found in binge eating disorder. Some argue the gender discrepancy is much less across all three eating disorders and that the current rate may be due to artifact as men are less likely to report and seek help for disordered eating behavior (National Eating Disorder Association).
Eating disorders have the highest mortality rate of all mental health disorders, with individuals diagnosed with anorexia nervosa having the highest mortality rate among the three eating disorders. Males may be at an increased risk for death because they are often diagnosed later due to the stigma associated with males and eating disorders. One interesting discrepancy between males and females’ development of eating disorders is weight history. Males who develop eating disorders are more likely to have been mildly to moderately obese at one point in their lives whereas women reported feeling fat but usually had a normal weight history (Andersen, 1999).
10.2.4.1 Societal variables. Probably the most prominent theory behind the development of eating disorders is the societal emphasis placed on physical attractiveness and thinness in women. This external variable is often compounded by the fact that women are interpersonally oriented, and thus value society’s opinion in their appearance. Unfortunately, society’s standards for thinness have grown to be more strict and unrealistic over the past years, largely driven by media, magazines, and television. In fact, frequent magazine reading was associated with an increase in unhealthy weight control measures among female adolescents (van den Berg et al., 2007). These findings have also been replicated in men who read magazines about fitness and muscularity (Hatoum & Belle, 2004).
With the rise in social media over the past decade, individuals have increased access to (often manipulated) images of “ideal bodies.” There has been a rise in studies examining the effects of social media on mental health, particularly body image and eating habits. Researchers continue to identify a positive correlational relationship between time spent on social media and eating/body image problems. More specifically, individuals who spent more time on social media also reported increase negative eating behaviors. These findings may be even more significant in individuals who frequently viewed fitspiration images (National Eating Disorder Association). Americans who spend two more hours a day on social media are exposed to more unrealistic ideals of beauty, weight loss stories, body shamming, etc. While research with regards to social media use and eating disorders have failed to examine differences between genders, it is hypothesized that similar to magazine reading, men are also affected by the increased social media use as well.
10.2.4.2 Familial variables. Societal pressures can also come from family and friends. Girls are more likely than boys to receive criticism from parents or close family members to lose weight; however, boys are often pressured by friends and family to gain muscle (Ata et al., 2007). Several studies have also identified that mothers of female eating disorder patients may actually have more impact on disordered eating habits that fathers. More specifically, direct negative maternal comments about weight and appearance may be a more powerful appearance than modeling of weight and shape concerns (Ogden & Steward, 2000). With that said, modeling does appear to have a more significant impact on elementary age girls’ weight and shape-related attitudes. Thus, modeling of negative body image at an early age may contribute to the development of an eating disorder while overt comments may exacerbate symptoms in older girls.
Family dynamics has also long been studied with regards to development of eating disorders. Although correlational at best, high levels of enmeshment, intrusive and overly hostile family environments are linked to eating disorders (Minuchin et al., 1978). Unfortunately, research in this area has not explored any differences in family dynamics and gender, therefore, we cannot determine whether enmeshment, intrusive, and overly hostile family environments impact the development of eating disorders in males.
10.2.4.3 Psychological factors. There are many individual factors such as low self-esteem, need for autonomy and control that have been linked to the development of eating disorders. Unfortunately, most if not all of the research with regards to individual characteristics is with an entirely female samples size. Therefore, it is difficult to determine if these factors also contribute to the development of eating disorders in men.
Individuals with eating disorders have a higher frequency of comorbid substance abuse than people who do not have eating disorders. Similarly, those who struggle with substance abuse also report increased disordered eating habits (Dunn, Larimer, & Neighbors, 2002). Interestingly, a gender discrepancy appears to exist with males reporting higher rates of comorbidity than females. More specifically, Costin and colleagues (2007) reported that roughly 57% of males with binge eating disorder struggle with substance abuse compared to only 28% of females with binge eating disorder. The high comorbidity between substance use and eating disorders has been linked to the use of stimulants to control weight. Due to the relationship between stimulants and weight management, treatment for the comorbid diagnoses is very difficult.
One area that is lacking in research but should be addressed is sexual orientation. Interestingly, homosexuality appears to be a risk factor for eating disorders for men, but not women. Furthermore, eating disorders are more common among homosexual men than heterosexual men, but not among lesbians compared to heterosexual women (Peplau et al., 2009). Future research on eating disorders and sexual orientation may help clinicians identify more effective treatment methods, particularly for male patients.
10.3. Suicide
Section Learning Objectives
- To gain a basic understanding of suicide rates in the US
- To increase understanding of the gender paradox in suicide
- To gain a better understanding of the various factors that contribute to suicidal ideation and suicide attempts
Suicide is ranked as the 10th leading cause of death for all ages in the United States. In 2016, it became the second leading cause of death for ages 10-34 and fourth leading cause for ages 35-54. While the government has made a targeted goal to reduce suicide rates by 2020, suicide rates across ages have steadily increased over the past few years (Office of Disease and Health Promotion, 2019). In fact, the age-adjusted suicide rate increased 33% from 10.5 per 100,000 standard population to 14.0 from 1999-2017. Statistics specific to gender identify a higher suicide completion rate in males (18/100,000) than females (11/100,000); however, the rate of suicide over the past decade has increased more drastically for females (53%) than males (26%).
While data continually reflects a discrepancy between genders, some argue that it may be artifact of biased data collection as women are more likely to report suicidal ideation/behavior than men. Conversely, death by suicide is more culturally acceptable for men than women, which also lends itself to another artifact of biased data collection.
10.3.1. Gender Paradox
When breaking down the statistics by gender, there are two trends that consistently hold true in Western cultures 1) females have a higher rate of nonfatal suicidal behavior and 2) males have a higher rate of suicide completion. Researchers have proposed several theories as to why this is the case. Intent of dying is one area that researchers have explored as one would naturally assume that if you have a report of more attempts but fewer completions, the true intent of the attempt would not be completion. This finding has not been consistently supported among researchers, with most studies reporting that the intent on dying is equal in men and women who engage in suicidal behaviors. (Denning, Conwell, King, & Cox, 2010). So, if women are just as intent as men on dying when engaging in suicidal behaviors, what else may explain this paradox?
The method of choice when engaging in suicide behaviors has long been a discussion in the gender paradox. Men are known to use more severe methods such as guns and hanging, whereas women are more likely to use drugs (over the counter and prescription) and carbon monoxide (see Table 10.1; Denning, Conwell, King, & Cox, 2010). Some argue that due to societal pressures, women place a higher emphasis on appearance, thus utilizing methods that ultimately do not affect their appearance.
Table 10.1. Suicide Methods
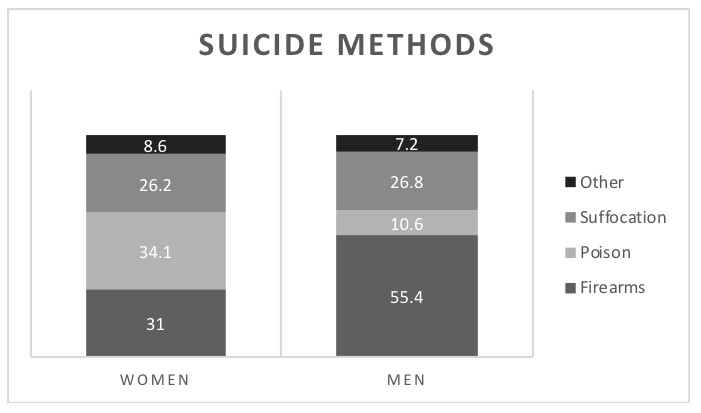
**Adapted from the Office of Disease Prevention and Health Promotion
The argument that choice of method reflects the intention to die has long been refuted in the literature as there is not a significant difference between men and women’s willingness to die with respect to suicidal behaviors (Nordentoft & Branner, 2008). With that said, because women are more likely to use methods more ambiguous methods (medications and poison), the actual rate of women’s suicides may be underreported as some deaths may be ruled “accidental.”
Cultural attitudes regarding masculinity and suicide has also been proposed as an explanation to the underreporting of men’s nonfatal behavior (Canetto & Sakinofsky, 1998). While suicide is not viewed as acceptable in most societies, it is viewed as more acceptable among men than women. Suicide itself is considered a more masculine behavior; however, suicide attempts are considered a more feminine behavior. Therefore, there may be an under representation of the number of suicide attempts/nonfatal behaviors in men due to the social stigma attached to nonfatal suicide behaviors.
10.3.2. Factors Related to Suicide
There are many factors that have been linked to suicide in both men and women. Most commonly, substance abuse and depression are linked to suicide in adults. One problem with the depression explanation is the possible cyclical relationship between depression and sucicide. More specifically, depression could lead to one engaging in suicidal behavior, however, a failed suicide attempt could also lead to depression. When exploring the relationship between depression and suicidal attempts, depressed men appear to be more at risk for serious suicidal behavior than women. Despite these findings, some researchers express caution in these statistics as they may be representative of artifact of women seeking help for mental illness more than men. This is evidenced by studies that found men who commit suicide are less likely than women who commit suicide to have used mental health services (Payne et al., 2008).
The one exception to the strong link between mental health and suicide attempts with regards to mental health diagnoses is substance abuse. Men who engage in substance abuse are more likely to commit suicide than women. One possible explanation of this finding is that substance abuse, particularly alcohol use, is a more socially acceptable way for men to alleviate symptoms of mental illness (Sher, 2006). Therefore, while women are more likely to seek professional help for mental health problems, men are more likely to “self-medicate” through the use of alcohol.
Relationships are also an important artifact in discussing the gender discrepancy of suicide rates. The risk of suicide is higher in unmarried, divorced, and widowed persons than married persons, with the overall risk being higher for men than women (Payne et al., 2008). Some argue that relationships reflect the lack of social support and that being married and thus receiving social support may be a protective factor against suicide in women. It has been further discussed that from a gender role perspective, women are also required to provide social support in families by taking care of the home, husband, and children, thus making them less likely to engage in serious suicidal behaviors.
In addition to relationships, financial status is also a strong predictor of suicidal behaviors. More specifically, individuals in lower socioeconomic status, those who are unemployed, as well as those that have financial problems are more at risk for suicide (Payne et al., 2008). These findings are more prominent in men than women. One possible explanation for the gender difference in suicidal rates with respect to financial status is related to gender roles. Men are typically viewed as the “bread winners” and the financial providers for the family. Therefore, when they are unable to fulfill this role, they may engage in more suicidal ideation and/or suicidal behaviors. This relationship may also be mediated by depressive symptoms, however, findings in support for this are inconsistent.
Finally, sexual orientation is also linked with suicidal behaviors, with sexual minority persons reporting increased suicidal ideation and attempts than heterosexuals (Payne et al., 2008). While women sexual minorities are at an increased risk for suicidal behaviors, non-heterosexual men are at an increased risk. This may be related to the greater stigma surrounding homosexuality in men, as homosexuality is viewed more acceptable in women than men.
10.4. Gender and Mental Health Treatment
Section Learning Objectives
- To understand factors that contribute to the gender discrepancy in seeking out mental health treatment
- To understand how Male Gender Role and Female Gender Role may impact men and women’s utilization of services
According to recent studies, only one-third of individuals who meet diagnostic criteria for a mental health disorder actually seek treatment, with women receiving treatment significantly more often than men (Andrews, Issakidis, & Carter, 2001). In fact, it is estimated that 1 in 3 women will receive mental health treatment at some point in their life compared to only 1 in 7 men (Collier, 1982). This should not be too surprising as women also seek out medical care more often than men. For example, men are more likely to utilize emergency services with respect to medical needs, whereas women are more likely to seek out appointments with a primary care physician (Husani, 2002; Rhodes & Goering, 1994). Models examining attitudes toward access of mental health treatment suggest that regardless of age and gender, negative attitudes toward treatment are largely responsible for the underutilization of mental health treatment.
Some argue that women have more psychological distress than men, hence the discrepancy in mental health treatment. Unfortunately, this is not the case as studies have shown that despite women seeking counseling more often than men, men report similar if not higher rates of distress than women (Robertson, 2001). Then maybe it’s lack of effectiveness in treatment? Again, it is suggested that although women are more likely to seek out treatment, men actually benefit more from the intervention (Hauenstein et al., 2006).
In attempts to better understand why individuals do and do not seek out mental health services, various models have been tested, including the suggestions in the previous paragraph. In more recent years, researchers have explored the impact of gender roles and gender stereotypes, and how they may impact an individual’s willingness to seek out treatment. We will briefly discuss how male gender role and feminist theory have impacted mental health treatment among both men and women.
10.4.1 Male Gender Role
Male gender role socialization suggests that in order for men to receive mental health treatment they need to set aside their masculine socialization to seek out this help (Robertson, 2001). More specifically, because of cultural implications of what are considered socially acceptable masculine behaviors versus female behaviors, men are less likely to report emotional distress and seek out help than their female counterparts. This theory was supported in a study that found a significant relationship between adherence to the male gender role and men’s help-seeking attitudes and behaviors (Good, Dell, & Mintz, 1989). More specifically, as men’s views became less traditional, their desire to seek out psychological help became more positive. Additional studies assessing masculine attitudes and desire to seek help supported these findings with men who scored high on gender role conflict also reported negative views of psychological help-seeking (Wisch, Mahalik, Hayes, & Nutt, 1995).
Gonzalez and colleagues (2005) examined models to determine how age, gender, and ethnicity/race impacted one’s attitude toward willingness to seek mental health treatment. Their findings indicated that younger individuals (under 24 years of age) were less willing to seek mental health treatment than their older counterparts. Similarly, men also had a more negative attitude toward mental health treatment and were nearly 50% less likely to seek mental health treatment as compared to females. Interestingly, when they examined an age by gender interaction, they found that younger males (under 24 years of age) were significantly less likely than females to seek mental health treatment. These findings also held consistent for older adults; however, when they examined willingness to seek mental health treatment between younger females (under age 24) and older male age groups (35-44 and 45-54), there was not a significant difference on willingness to seek mental health treatment.
These findings support gender role socialization as women are conditioned to be more accepting of the help-seeking role, and therefore, are more likely to seek assistance when needed. This is also indicted through studies that find men who report more traditional sex role orientation and independence as having more negative attitudes toward seeking mental health treatment (Ortega & Alegria, 2002).
10.4.2. Feminist Psychotherapy
Feminist theory grew out of the women’s movement in the 1960’s. During this grassroots movement, women identified psychological structures of evaluation as contributing to women’s oppression and subordination in society, while also offering scientific rationale for women’s secondary social status. In efforts to combat these issues, feminist psychotherapy was founded. The goal of feminist psychotherapy is to identify gender related challenges/stressors that women face as a result of bias, stereotypes, oppression, and discrimination. Through an equal relationship between the therapist and the patient, feminist psychotherapy helps patients to understand social factors that contribute to their issues, help them discover their own identity, and help build on personal strengths. Although labeled as feminist theory, any group that has been marginalized can benefit from feminist psychotherapy as the main goal of treatment is to identify individual strengths and utilize them to feel more powerful in society (Psychology Today).
According to Lenore Walker, there are six tenants of feminist psychotherapy:
- Egalitarian relationships: the equal relationship between patient and therapist models personal responsibility and assertiveness for other relationships
- Power: patients are taught to gain and use power in relationships
- Enhancement of strengths: patients are taught to identify their own strengths and use them effectively
- Non-pathology oriented: patient’s problems are seen as coping mechanisms and viewed in their social context
- Education: patients are taught to recognize their cognitions that are detrimental and encouraged to educate themselves for the benefit of all
- Acceptance and validation of feelings: patients are encouraged to self-disclose to remove the we-they barrier of traditional therapeutic relationships
As stated above, the goal of feminist psychotherapy is to encourage change and establish empowerment in women and minority groups. One way therapists do this is by addressing gender issues as they can cause psychological distress and shape one’s behavior. If you think about it, we are all affected and influenced by stigmas and stereotypes. Feminist psychotherapy aims to help patients of minority groups to identify these stigmas and stereotypes, while simultaneously challenge them in attempts to help improve the patient’s overall mental health.
Of course, as with all types of treatments, there are some limitations and criticisms. While the goal of feminist theory is to provide strength and empowerment to women and minority groups, some therapists may take this too far. Therapists that are too strong in their feminist beliefs may become militant in their views, thereby persuading patients. A feminist therapist should be supportive and challenge a patient’s thoughts, not forcefully change a patient’s viewpoint. Additionally, some argue that by taking a feminist view on treatment and society, the therapist is not neutral in their beliefs, thus predisposing patients to blame society for their issues rather than taking ownership. As with all types of treatments, there are limitations. It is important that the patient identifies a treatment method that is comfortable to them, as the ultimate goal is to improve their mental health well-being.
Module Recap
In Module 10, we discussed the methodological artifacts from both clinician and reporting biases that may contribute to the gender differences among prevalence rates among mental health disorders. In keeping some of these artifacts in mind, we also discussed gender differences in rates of the most common psychological disorders- depression, anxiety, PTSD and eating disorders, as well as the biological, cognitive, psychological, and societal factors that contribute to these gender differences. It is important that you are able to identify these different factors as they contribute to differing rates of mental health disorders between men and women. We also discussed suicide and the gender paradox that although men complete more suicides, women are more likely to engage in nonfatal behaviors. We also identified the different methods men and women used when engaging in suicidal behaviors. The module concluded with a brief overview of how gender may impact one’s willingness to seek out mental health treatment and how feminist psychotherapy may help women and other minority groups address societal influences.